COHSE - Join The Resistance Banner - Nottingham Thursday 4th February 1988
1,000 strong march in freezing weather from Forest Recreation Site to Market Square
photo Martin Jenkinson (Click picture to enlarge)










 1988 Nurses Strike
1988 Nurses Strike Ken Livingstone MP for Brent East with COHSE placard at the opening of the new Psychiatric Unit on the Central Middlesex Hospital site Circa early 1989. (With Barbar Young).
Ken Livingstone MP for Brent East with COHSE placard at the opening of the new Psychiatric Unit on the Central Middlesex Hospital site Circa early 1989. (With Barbar Young).


LES MISERABLES
French Nurses Strikes
When the French authorities used tear-gas and water-cannon on a nurses' demonstration last month, injuring several protestors, it served only to enrage further a profession already at the end of its tether.
Nursing in
of work have led to a veritable hemorrhage from the profession. There are
some 600 000 French nurses but only 280 000 of them are working. More
than half have quit nursing for better- paid jobs and the country's health
service desperately needs them back.
The public are backing them, with 78% of those questioned in a poll saying nurses were right to go on strike. And nurses staging a day-and-night sit-in outside the Ministry of Health have been overwhelmed by offers of support — not to mention croissants and coffee — from local residents and from passers-by.
The doctors are on their side too. On October 24 the nurses staged Operation Infirmiere Zero — a one-day strike during which, by agreement, doctors
took on nursing duties. To keep up the pressure, the nurses are staging a
one-hour walkout every day.
Staff shortages and the extra pressures that leads to are the main grievances, but pay is a real source of discontent too. French nurses are on a pay scale with public sector workers and earn between £750 and £820 a month. However, they want recognition that their work carries more responsibility than postal or
refuse workers and so they are asking to come off that scale and boost their earnings to £950 a month.
The profession also wants improved supplements for working unsocial hours and they regard the £6 extra they are paid for doing a night shift as an insult.
The 1988 dispute led to the formation of La Coordination Nationale Infirmiere, the first-ever union in
Meanwhile, a recent headline in a daily paper sums up the current black mood. 'Infirmiere, un travail de chien.' 'Nursing is dogs' work.'
Janet Snell
Nursing Times
NOTE
the CGT is still the premier union in
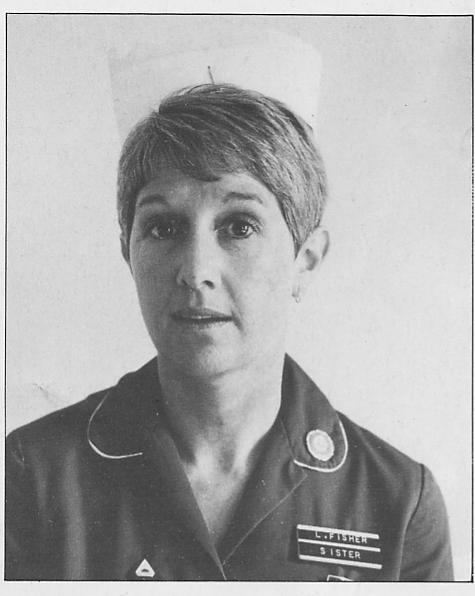
Lesley Fisher, I work as a night sister at
cutting taxes rather than increasing health service funding. They are amazed at the hypocrisy of a government that, in the same week as it claims to care about shortage of specialist nurses, attempts to cut special duty payments. Nurses are incensed by Mrs Thatcher's speech in which she insisted that it is we nurses, driven to this action and at the end of our tether, who are guilty of ruining the NHS.
NURSING TIMES FEBRUARY 3.VOL 84, NO 5. 1988
Note
Lesley Fisher former UNISON national health care sector Chair UNISON London health care sector chair until 2007 - still 85% UNISON membership in her Haringey (St Ann's Hospital) branch
Born in Belfast 19 October 1946 , , came to Addenbrookes, Cambridge to train as a nurse, later worked at the Elizabeth Garratt Anderson (EGA) where she be came involved in NUPE, later worked at Wood Green and Southgate hospital) and St Ann's Hospital